Body Balance Quarterly #1
Topic One
Knee Troubles???
Thinking Surgery For Knee Osteoarthrits?????
Here is the current research:
Over the last few years two studies in particular have adjusted the way we treat patients who enter the clinic with osteoarthritis related knee issues. If we are able to assess this patient case load prior to any further consultation we discuss current research and the importance of the findings and results of physiotherapy intervention verses undergoing surgical intervention.
Although arthroscopic surgery has been widely used for treatment of osteoarthritis of the knee, scientific evidence to support its effectiveness was lacking. Two articles have more recently been released looking at: 1. arthroscopic surgery itself verses a placebo surgery and 2. arthroscopic surgery with physiotherapy intervention verses physiotherapy intervention on its own.
The results were quite interesting.
The two papers of interest are discussed below:
- (A Controlled Trial of Arthroscopy Surgery for Osteoarthritis of the knee – Moseley J.B et al. New England Journal of Medicine. Vol. 347,No 2, July 11, 2002 )
This study specifically looked at a Veterans Affairs Hospital in which only men participated as the testing subjects. All participants in the study underwent either a sham or real surgery – blinded to which group they were in (arthroscopic debridement, arthroscopic lavage, or placebo surgery – in which the arthroscopic debridement procedure was simulated). Data was collected over a 24 month period and all patients received the same walking aids, graduated exercise program and pain killers.
RESULTS: Showed strong evidence that arthroscopic lavage with or without debridement is not better than and appears to be equivalent to a placebo procedure in improving knee pain and self reported function.
Taking these findings into consideration further research was performed by Kirkley et al., which worked to fix the previous studies methodological issues.
- (A Randomized Trial of Arthroscopic Surgery for Osteoarthritis of the Knee –Kirkley et al. New England Jounral of Medicaine. Vol.359 2008 )
This study looked at patients who were randomly assigned to surgical lavage and arthroscopic debridement together with optimized physical therapy and medical therapy or to treatment with physical and medical therapy alone. With the inclusion criteria listed as such – 18 years or older with idiopathic (unknown cause) or secondary osteoarthritis of the knee, with grade 2, 3,or 4 radiographic severity
Exclusion criteria was – any large mensical tears, inflammatory or post infections arthritis, previous arthroscopic treatment for the knee Osteoarthritis, greater than 5 degrees varus or valgus deformity, previous knee trauma, grade 4 osteoarthritis in two compartments, previous corticosteroid injection with in the previous 3 months, major neurological deficit, serious medical illness, pregnancy and inability to provide informed consent.
Patients were randomly assigned to receive optimized physical therapy and medical therapy alone or to receive both optimized physical and medical therapy and arthroscopic treatment. Optimized physical therapy and medical therapy were both initiated 7 days after surgery and followed an identical program in both groups.
RESULTS: Arthroscopic surgery for Osteoarthritis of the knee provides no additional benefit to optimized physical and medical therapy.
As physiotherapists it is our job to not only supply the current research available to you on these types of surgeries but provide programs to help you have the best functional outcome that we can. These two studies provide strong evidence and results recommending more of a physical strength building program over that of performing Arthroscopic surgery as a first choice for those struggling with mild to moderate levels of osteoarthritis. Needless to say reading this you must keep in mind the exclusion criteria for these studies – i.e., if worse non-traumatic mensical tears are present over that of Osteoarthritis severity arthroscopic surgery has still been controversial but results have been found to be of benefit in 1/3 of the population.
Further research on this specific population can be found in the article – as an online source – Is Arthroscopic Surgery beneficial in treating non-traumatic degenerative medial mensical tears? A five year study.
If you have further questions about this research, don’t hesitate to ask one of the Physiotherapists in our office.
Topic Two
Other Options For Knee Oa???
Valgus Knee Braces (For Knocked Knee Problem) ???
Improvements in function have been reported in patients with Osteoarthritis following knee bracing for durations between 6 months and 12 months. Although the bracing achieves effective unloading of the inside compartment of the knee and offers potential for improving outcome in patients with knee osteoarthritis – beyond being an expensive purchase – the success of this intervention relies upon the patient being prepared to wear the brace continually.
Valgus knee braces are bulky, potentially uncomfortable and might not be a practical daily solution for many patients.
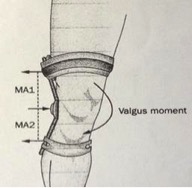
Figure 4:
Schematic diagram illustrating how values bracing counteracts the external adduction moment acting about the knee during walking. The brace applies points of force at three locations (indicated by arrows), which create MA1 and MA2, and result in a values moment about the knee. The red dotted line indicates the length of the two separate moment arms: Ma1 and MA2 (distance from outer arrow to center arrow). Abbreviation: MA, moment arm.
Walking Aids???
Cane use in conjunction with a slow walking speed decreases the biomechanical load experienced by the lower limb. The use of a cane and walking slowly could therefore be a simple and effective intervention for patients with osteoarthritis.
Keeping in mind the cane must be placed in the opposite hand to the symptomatic knee.
Flexible shoe verses stability shoe ???
Wearing shoes that have a thin and flexible sole and little to no heel, offers a potentially useful strategy for effectively modifying the biomechanical factors influencing progression of osteoarthritis.
Thin soled, flexible shoes seem to be beneficial for reducing joint loads compared to shoes with thicker soles – why?? Thinner soles provide a shorter stride and smaller ranges of motion in knee and ankle joints.
Reference/Source – Conservation Biomechanical Strategies for Knee OA. Neil D. Reeves and Frank L Bowling. Nature Review/Rheumatology Vol 7, 2011.