We are closed for the civic holiday on Monday.
Body Balance Quarterly #4
With the return of warmer weather, comes the return to outdoor activities.
The Spring/Summer edition of the BBQ features some ideas to help you stay fit with gardening, prevent stiffness and pain from those long road trips, and try to help you sift through whether to invest in a brace.
DRIVING:
Have you ever felt stiff and sore in your back, neck or knees after a long car ride? Has this soreness taken away some of your enjoyment on your trip?
Here are a few ideas you can easily incorporate to try to help:
- Pacing – As much as you may want to just “bite the bullet” and make the trip in one shot, it is very important to take breaks. Ideally, every 20-30 minutes. Realistically, this may not be manageable; but, the take home message is to at the very least, take more breaks than you may have before.
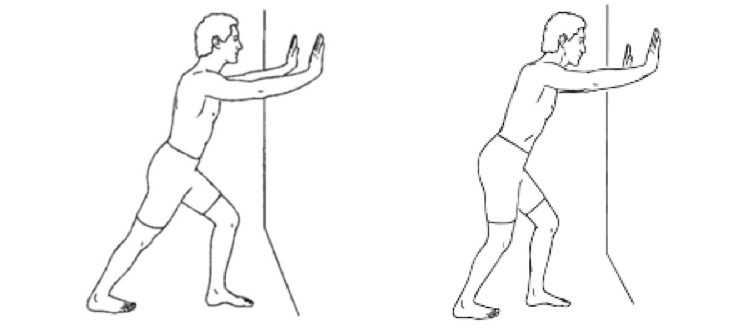
- Posture – Everything you try to do to keep good sitting posture is just as important in the car. Most car seats encourage an increased “C” curvature in the low and mid back because of the angle of the seat.

Proper positioning of the car seat should look like the green line in this picture:

As you can see, the 2 don’t match. Most cars now have multiple ways you can adjust the seat. We suggest you work with these to try to get as close to the “right” picture as possible. Also, if more adjustment needs to occur, we suggest adding a folded blanket/towel or cushion at the back half of the seat cushion to get the seat pan closer to neutral. Also, a small roll at the back can help to bring the back rest straighter. But, remember that safety is always the most important. That means that if you have to place yourself too close to the airbag or your head is too close to the roof of the car to be safe driving, then you may have to just try to get close to neutral posture and accept that perfection won’t be possible.
How Do I Minimize Pain With Gardening? :
If you love flowers or having fresh veggies grown in your back yard, it is important to remember that, physically, gardening involves postures that are not ideal for our body. That’s why we suggest you incorporate a few of the following ideas:
- Pacing – Our body prefers to be moving. It is not a good idea to be in a certain posture for more than 30 minutes at a time. The ideal situation is to plan and structure periodic rest breaks into your day. Set the timer on your phone as a reminder and then stop your task to do some walking or change from a bending task to one where you are standing.
- Proper Lifting – If you have to carry plants or mulch or using the wheel barrel, we suggest you make sure you remember your own personal limits. Just accept that some things you plan to carry might be too heavy for you. Ask someone to help or if you can, split what you are lifting into smaller weights and make more frequent trips.
- Proper carrying – Again, we suggest you don’t carry more than you can safely handle. Remember to keep what you are carrying close to your body. If you have to do multiple trips with the watering can, remember to switch which arm you are carrying it with to keep your muscles balanced.
- Hydration – Don’t forget to stay hydrated. Cells in the body need water to function properly. Remember to replenish what you lose!
To Brace or Not To Brace:
This is a common question we are often asked in the clinic. It is difficult for a consumer to sift through all the competing brands and gadgets that are currently out on the market or what may show up with a google search.
There are numerous factors to take into consideration when deciding if a brace will help and that is only half the challenge. Once you decide to get a brace, you must now try to decide what to purchase. In the next few editions, we will profile various physical injuries/problems and try to give you some insight into what to consider.
In this edition, we profile elbow bracing. When the tendons at the elbow get inflamed from overuse or repetitive movements, pain can develop at the inner elbow (also known as golfer’s elbow) or the outer elbow (also known as tennis elbow). In our professional experience, these problems respond well to using a brace; however, we do stress that you don’t try to self diagnose yourself and make sure you get the proper advice on whether this is your proper diagnosis.
The brace used for these problems is commonly called a “tennis elbow cuff.” The idea behind it is to create a pressure point about an inch away from the area of pain in the elbow. This allows you to continue to use the muscle from that point; but, reduces the amount of force going through the tendon attachment at the elbow (where the pain is). If it is doing what it is supposed to, there should be an immediate decrease in pain after the cuff is in place and you try to use the arm and hand. You should make sure that you don’t have it on so tight that it affects your circulation. Also, you should consider it’s comfort level because some are made with hard material, which can irritate the skin when bending the elbow.
If there is no immediate benefit, we don’t recommend using one.
Here is an example of what one looks like:

We do not recommend that people self diagnose their injuries and the advice provided is not to replace obtaining a proper assessment and diagnose by a qualified health care professional.
Body Balance Quarterly #3
2016 has been off to a slow start regarding poor weather conditions and we are very fortunate to that when it comes to shovelling snow and the protection of our backs. We are reminded however that winter is not quite over and spring snow tends to be quite heavy and more difficult to move.
Remember these quick tips to promote safe shovelling:
- Tip # 1.
If you experience pain of any kind, stop immediately and seek assistance. - Tip # 2.
Choose a snow shovel that is right for you!- Be sure that your shovel has a curved handle, as this enables you to keep your back straighter when shoveling.
- Obtain a shovel with an appropriate length handle. The length is correct when you can slightly bend your knees, flex your back 10 degrees or less, and hold the shovel comfortably in your hands at the start of the “shoveling stroke”.
- A plastic shovel blade will generally be lighter than a metal one, thus putting less strain on your spine.
- Sometimes, a smaller blade is better than a larger blade. Although a small blade can’t shovel as much, it avoids the risk of trying to pick up a too heavy pile of snow with a larger blade.
- Tip # 3.
Push the snow, do not lift it. Pushing puts far less strain on the spine than lifting. - Tip # 4.
Be sure your muscles are warm before you start shoveling. Cold, tight muscles are more likely to sprain or strain than warm, relaxed muscles. - Tip # 5.
When you grip the shovel, make sure your hands are at least 12 inches apart. By creating distance between your hands, you increase your leverage and reduce the strain on your body. - Tip # 6.
“If you must lift the snow, lift it properly. Squat with your legs apart, knees bent and back straight. Lift with your legs. Do not bend at the waist. Scoop small amounts of snow into the shovel and walk to where you want to dump it. Holding a shovel of snow with your arms outstretched puts too much weight on your spine. Never remove deep snow all at once; do it piecemeal. Shovel and inch or two; then take another inch off. Rest and repeat if necessary.” In addition to these comments, remember to move your feet rather than twisting. - Tip # 7.
Never throw snow over your shoulder. - Tip # 8.
Remember that wet snow can be very heavy. One full shovel load can weigh as much as 25 pounds. - Tip # 9.
Pace yourself by taking frequent breaks to gently stretch your back, arms and legs. - Tip #10.
Consider buying a snow-blower. When used correctly, a snow-blower will put far less strain on your back than snow shoveling.
SOURCE OF INFOMATION: http://www.coloradospineinstitute.com/subject.php?pn=wellness-snow-shoveling
Topic of interest – Paediatric Sports Injury
A common injury for Paediatric sports that involve a lot of jumping (basketball, volleyball) is the pain and inflammation caused by “jumpers knee”. The following stretching recommendations are not intended as treatment but are advised to be done in the prevention of injury.
If you suffer from constant pain below the knee or experience episodes of inflammation and pain in relation to the sport that you are participating in; it is recommended that you consult your Physician or Health Care Provider to determine the course of treatment that is best for your injury.
Stretching and strength exercises should not be done or pursued in the presence of pain. It is important to stop any exercise in the presence of pain and consult your Health Care Practitioner.
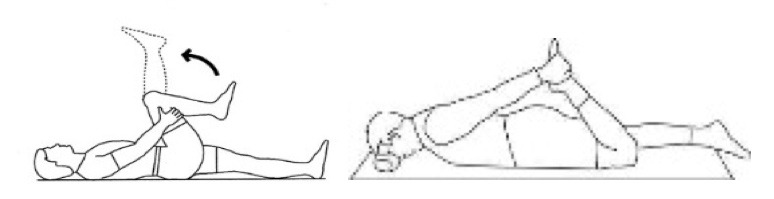
Key point #1
Maintain ankle mobility – Tight calf muscles or poor ankle mobility have a negative impact on the knee. In picture one the back leg remains straight and in picture two the back leg bends at the knee. These stretches address different muscle groups and assist in the prevention of stiffness at the ankle.
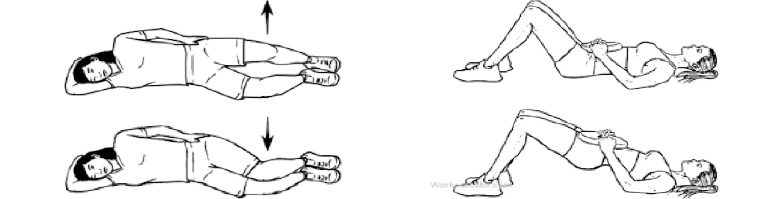
Key point #2
Maintain proper range of motion in the Quads and Hamstring muscles – These muscles have a direct impact on the mechanics of the knee and maintaining good flexibility in these muscles goes a long way in injury prevention
Key point #3
Strengthen the muscles of the hip – It is especially important to strengthen the gluteal muscles and abductor muscles of the hip as these muscles help to control the stability of the femur.
Spring is Near!
This Issue started with reminders on stretches and injury prevention for shovelling and we would like to end it on a more inspiring topic, GOLF! Yes, golf season is getting closer and closer and that’s a lot better to think about than shovelling so if golf is your thing check out this link for a few key points on stretching before you get out and swing that golf club for the first time in four or five months!
Body Balance Quarterly #2
Head Injury, Helmets and How to Treat Brain and Vestibular Problems
In this Issue:
- Helmet Safety
- Dizziness, Balance and Vertigo Treatment
- Body Balance Bursary
HELMET USE AND SAFETY
In our office, we are seeing more and more people for treatment following concussions and other head injuries. Whether this is because more injuries are occurring or whether health care practitioners and the public are better educated to recognize them, is still up for debate; however, the fact remains that head injury is a growing problem.
The best way to treat a head injury is to never have one in the first place. That is why proper helmet use is so important.
Here is a list of a few tips for getting the proper helmet.
- Understanding How A Helmet Works
The purpose of the shell is to keep the shape of the helmet, distribute impact, protect against sharp objects penetrating the head and to help skid across the ground.
The foam on the inside is designed to “break”. When you hit the ground or surface, your head continues to move within the helmet and crushes the foam inside. The foam then absorbs the impact so the force of the impact on your head lessens.
- Get the Proper Helmet for the Proper Use/Goal
Helmets have specific designs based on which sport you participate in. They vary in shape based on what part of the head needs protection (ie. Bike helmets are designed for protection from impact at the front and sides, whereas skateboarding helmets are designed to protect the head from impact on all sides.)
In addition, there are helmets designed specifically to protect from a high impact force – known as “single impact helmets” (ie. Skiing), versus ones designed to sustain repeated smaller forces – “multiple impact helmets” (ie. Hockey).
Keep these issues in mind when deciding which helmet to buy and use. HELMETS ARE NOT INTERCHANGEABLE BETWEEN SPORTS.
- Replace the Helmet as Recommended/Required
Single impact helmets should always be replaced after one crash.
Multiple impact helmets are designed to take smaller, repetitive impacts before needing to be replaced.
Even without a crash, helmets are not designed to last forever. The poly-styrene liners should be replaced every 5 years and the crushable liners should be between 1.5 cm and 3.0 cm thick.
You should also consider temperature conditions and the amount of sweating because this affects the inside foam of the helmet and may be another deciding factor in replacing the helmet.
- Get the Proper Fit
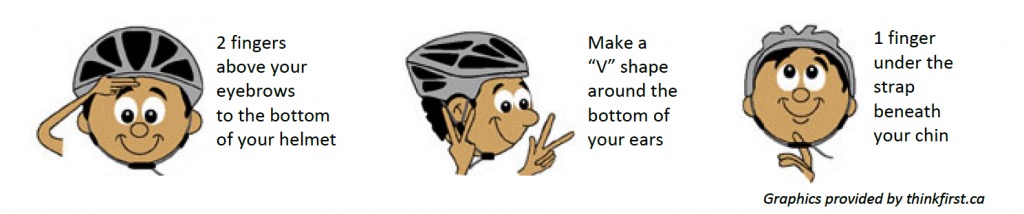
The Newfoundland and Labrador Brain Injury Association website suggests using the “2-V-1 Rule”:
- The helmet should sit 2 fingers above brow line for children, 1 finger for adults
- Straps should form a “V-shape” below each ear
- 1 finger should fit snugly between the chin and helmet buckle (loose enough that it doesn’t pinch the chin and tight enough that the buckle touches the skin)
It is important to keep the straps firm and snug so the helmet doesn’t move or shift to expose the head.
HELMET DO’S AND DON’TS:
DO
- Check inside the helmet for certification stickers, because not all helmets have the same legislated standards.
- The most recognized association at this time is the Canadian Standards Association (CSA) certification.
- Remember to wear and use the helmet as instructed by the manufacturer. For example, hockey helmets have an expiry date.
DON’T
- Use stickers, tape or paint on the helmet as it can hide cracks or dents, which are signs that the helmet must be replaced.
- Don’t leave the helmet outside because weather and temperature can affect the materials.
- Don’t toss helmets on the ground as that is an impact force and can damage or weaken the helmet.
DIZZINESS, BALANCE, VERTIGO
- Do I feel unsteady?
- Do I feel as if the room is spinning around me?
- Do I lose my balance and fall?
- Do I feel as if I am falling?
- Do I feel lightheaded or as if I might faint?
- Do I have blurred vision?
- Do I ever feel disoriented, such as losing my sense of time or where I am?
If you answered “yes” to any of these questions, you may have a disorder with your vestibular system. While it is not uncommon for everyone to experience some issues of dizziness; people who benefit from vestibular rehab experience these symptoms to a greater extent, which can severely impact on one’s quality of life and ability to perform in society.
What Is a Vestibular Disorder?
The vestibular system is what helps your body adjust to changes in your environment. Information about your environment from vision, proprioception (touch receptors) and the inner ear is sent to the brainstem. The brainstem collects this information, processes it, figures out what the body has to do to adjust, and then sends feedback to steady the vision, adjust muscle position/centre of gravity and balance. When it works properly, these adjustments are done at remarkable speed. If the vestibular system is not working, conflicting information between these components occurs and we end up with dizziness, vertigo or disequilibrium.
Symptoms/Definitions:
- Dizziness – lightheadedness, faintness
- Vertigo – sensation of the room spinning/moving
- Disequilibrium – loss of steadiness
Some examples of what patients describe are the following:
- Feeling like they drift to one side when walking
- Uncomfortable in stores
- Fatigue
- Difficulty reading
- Difficulty watching TV or using a computer
What Causes Vestibular Disorders?
Vestibular disorders can be as a result of:
- Head injuries
- Medication
- Disease
- Viral
- Aging
- Inner ear deficit
What can get confusing is that similar symptoms can also be produced by neurological injuries/disorders (Parkinson’s, stroke), circulation problems, eye problems, etc.
Treatment:
As mentioned previously, there can be a variety of causes for vestibular disorders and to make the situation more complex, sometimes the symptoms we experience may not be related to the vestibular system at all. That is why it is so important to have a qualified physiotherapist perform a comprehensive assessment. Specifically, a physiotherapist who has taken advanced level training and has experience in vestibular rehabilitation.
Because of how complex dizziness and vertigo treatment is, it is not possible to condense everything and everyone’s problems into this one article; but, the take home message is to make sure people are aware that, in a number of cases, there are options available to help you feel better and that these are not simply issues you have to “live with”.
For more detailed information, we suggest you visit the website www.vestibular.org.
Don’t forget to visit our Facebook page for contests all year long!
Body Balance Quarterly #1
Topic One
Knee Troubles???
Thinking Surgery For Knee Osteoarthrits?????
Here is the current research:
Over the last few years two studies in particular have adjusted the way we treat patients who enter the clinic with osteoarthritis related knee issues. If we are able to assess this patient case load prior to any further consultation we discuss current research and the importance of the findings and results of physiotherapy intervention verses undergoing surgical intervention.
Although arthroscopic surgery has been widely used for treatment of osteoarthritis of the knee, scientific evidence to support its effectiveness was lacking. Two articles have more recently been released looking at: 1. arthroscopic surgery itself verses a placebo surgery and 2. arthroscopic surgery with physiotherapy intervention verses physiotherapy intervention on its own.
The results were quite interesting.
The two papers of interest are discussed below:
- (A Controlled Trial of Arthroscopy Surgery for Osteoarthritis of the knee – Moseley J.B et al. New England Journal of Medicine. Vol. 347,No 2, July 11, 2002 )
This study specifically looked at a Veterans Affairs Hospital in which only men participated as the testing subjects. All participants in the study underwent either a sham or real surgery – blinded to which group they were in (arthroscopic debridement, arthroscopic lavage, or placebo surgery – in which the arthroscopic debridement procedure was simulated). Data was collected over a 24 month period and all patients received the same walking aids, graduated exercise program and pain killers.
RESULTS: Showed strong evidence that arthroscopic lavage with or without debridement is not better than and appears to be equivalent to a placebo procedure in improving knee pain and self reported function.
Taking these findings into consideration further research was performed by Kirkley et al., which worked to fix the previous studies methodological issues.
- (A Randomized Trial of Arthroscopic Surgery for Osteoarthritis of the Knee –Kirkley et al. New England Jounral of Medicaine. Vol.359 2008 )
This study looked at patients who were randomly assigned to surgical lavage and arthroscopic debridement together with optimized physical therapy and medical therapy or to treatment with physical and medical therapy alone. With the inclusion criteria listed as such – 18 years or older with idiopathic (unknown cause) or secondary osteoarthritis of the knee, with grade 2, 3,or 4 radiographic severity
Exclusion criteria was – any large mensical tears, inflammatory or post infections arthritis, previous arthroscopic treatment for the knee Osteoarthritis, greater than 5 degrees varus or valgus deformity, previous knee trauma, grade 4 osteoarthritis in two compartments, previous corticosteroid injection with in the previous 3 months, major neurological deficit, serious medical illness, pregnancy and inability to provide informed consent.
Patients were randomly assigned to receive optimized physical therapy and medical therapy alone or to receive both optimized physical and medical therapy and arthroscopic treatment. Optimized physical therapy and medical therapy were both initiated 7 days after surgery and followed an identical program in both groups.
RESULTS: Arthroscopic surgery for Osteoarthritis of the knee provides no additional benefit to optimized physical and medical therapy.
As physiotherapists it is our job to not only supply the current research available to you on these types of surgeries but provide programs to help you have the best functional outcome that we can. These two studies provide strong evidence and results recommending more of a physical strength building program over that of performing Arthroscopic surgery as a first choice for those struggling with mild to moderate levels of osteoarthritis. Needless to say reading this you must keep in mind the exclusion criteria for these studies – i.e., if worse non-traumatic mensical tears are present over that of Osteoarthritis severity arthroscopic surgery has still been controversial but results have been found to be of benefit in 1/3 of the population.
Further research on this specific population can be found in the article – as an online source – Is Arthroscopic Surgery beneficial in treating non-traumatic degenerative medial mensical tears? A five year study.
If you have further questions about this research, don’t hesitate to ask one of the Physiotherapists in our office.
Topic Two
Other Options For Knee Oa???
Valgus Knee Braces (For Knocked Knee Problem) ???
Improvements in function have been reported in patients with Osteoarthritis following knee bracing for durations between 6 months and 12 months. Although the bracing achieves effective unloading of the inside compartment of the knee and offers potential for improving outcome in patients with knee osteoarthritis – beyond being an expensive purchase – the success of this intervention relies upon the patient being prepared to wear the brace continually.
Valgus knee braces are bulky, potentially uncomfortable and might not be a practical daily solution for many patients.
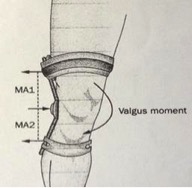
Figure 4:
Schematic diagram illustrating how values bracing counteracts the external adduction moment acting about the knee during walking. The brace applies points of force at three locations (indicated by arrows), which create MA1 and MA2, and result in a values moment about the knee. The red dotted line indicates the length of the two separate moment arms: Ma1 and MA2 (distance from outer arrow to center arrow). Abbreviation: MA, moment arm.
Walking Aids???
Cane use in conjunction with a slow walking speed decreases the biomechanical load experienced by the lower limb. The use of a cane and walking slowly could therefore be a simple and effective intervention for patients with osteoarthritis.
Keeping in mind the cane must be placed in the opposite hand to the symptomatic knee.
Flexible shoe verses stability shoe ???
Wearing shoes that have a thin and flexible sole and little to no heel, offers a potentially useful strategy for effectively modifying the biomechanical factors influencing progression of osteoarthritis.
Thin soled, flexible shoes seem to be beneficial for reducing joint loads compared to shoes with thicker soles – why?? Thinner soles provide a shorter stride and smaller ranges of motion in knee and ankle joints.
Reference/Source – Conservation Biomechanical Strategies for Knee OA. Neil D. Reeves and Frank L Bowling. Nature Review/Rheumatology Vol 7, 2011.
We’re excited to show you our brand new website. Please take a look around, and check back here for regular news updates!